Breast augmentation with implants
For breasts that have lost volume but have not sagged. Implant placement without altering breast position. The most common implant surgery — approximately 80% of implant patients.
Breast augmentation with implants is appropriate when the nipple-areola complex sits at or above the inframammary fold and points forward — anatomic indicators that the breast has lost volume but not significantly sagged. Surgery places implants under the muscle (submuscular), over the muscle (subglandular), or in dual-plane configuration. Five orthogonal implant decisions (type, shape, profile, surface, brand) are made together with the surgeon. Recovery 7-14 days for office work, 6-8 weeks for full physical activity. Final result emerges at 3-6 months.
Anatomic candidacy
The single most important question in implant surgery is: do you need a lift, or only an implant? Two surgeries — augmentation alone vs augmentation + mastopexy — produce very different outcomes for very different anatomy. Choosing the wrong one creates dissatisfaction that cannot be corrected without a second operation.
The nipple-fold relationship
The most reliable anatomic test:
- Nipple at or above the inframammary fold, pointing forward: implant alone is appropriate. Approximately 80% of patients seeking implants.
- Nipple at the inframammary fold, pointing slightly down: borderline. Some surgeons offer implant alone with a strong implant and accept slight residual sagging; others recommend lift. Dr. Erdal's practice typically recommends lift in this borderline case.
- Nipple below the inframammary fold or pointing significantly down: mastopexy required. Implant alone will exaggerate the sagging.
The most common patient error: hoping that a larger implant will lift sagging breasts. It does not. A larger implant adds volume to whatever shape the breast already has — including the sagging. Volume without lift makes the result worse, not better.
Other anatomic factors
- Skin elasticity — younger patients with elastic skin tolerate larger volume changes; older patients or those with prior pregnancies/weight loss may need restraint.
- Chest base width — limits maximum implant width (cannot exceed your chest base).
- Existing breast tissue volume — affects what surface coverage you have over the implant.
- Body proportion — large implants on a small frame look prominent; smaller implants on a tall frame may look subtle.
- Goal expectations — subtle natural look (most common in modern practice) vs prominent fuller-than-baseline look.
Implant decisions
Five orthogonal decisions every implant carries:
| Decision | Options | Most common for primary augmentation |
|---|---|---|
| Type | Silicone gel, cohesive gel, saline, structured saline, B-Lite | Cohesive gel |
| Shape | Round, anatomical (teardrop), ergonomic | Round (or ergonomic) |
| Profile | Low, moderate, moderate-plus, high, extra-high | Moderate-plus or high |
| Surface | Smooth, microtextured, macrotextured, polyurethane-coated | Microtextured (in EU/UK) |
| Brand | Motiva, Mentor, Natrelle/Allergan, Polytech, Sebbin, Nagor | Brand-specific selection based on availability and surgeon experience |
Each decision has a dedicated reference page (silicone gel, cohesive gel, round, anatomical, moderate profile, high profile, microtextured, Motiva, etc.). Read individually for granular detail; the consultation discusses the specific combination for your anatomy.
The brand-neutral approach. This practice carries multiple implant brands. The selection for your specific case is based on anatomic fit, your priorities (texture, shape, longevity, warranty), and surgeon experience with each brand — not on commercial relationships. If a particular brand is suggested, you can ask "why this brand for me specifically?" — the answer should reference your anatomy and goals, not generic brand marketing.
Placement options
| Placement | Description | Strengths | Limitations |
|---|---|---|---|
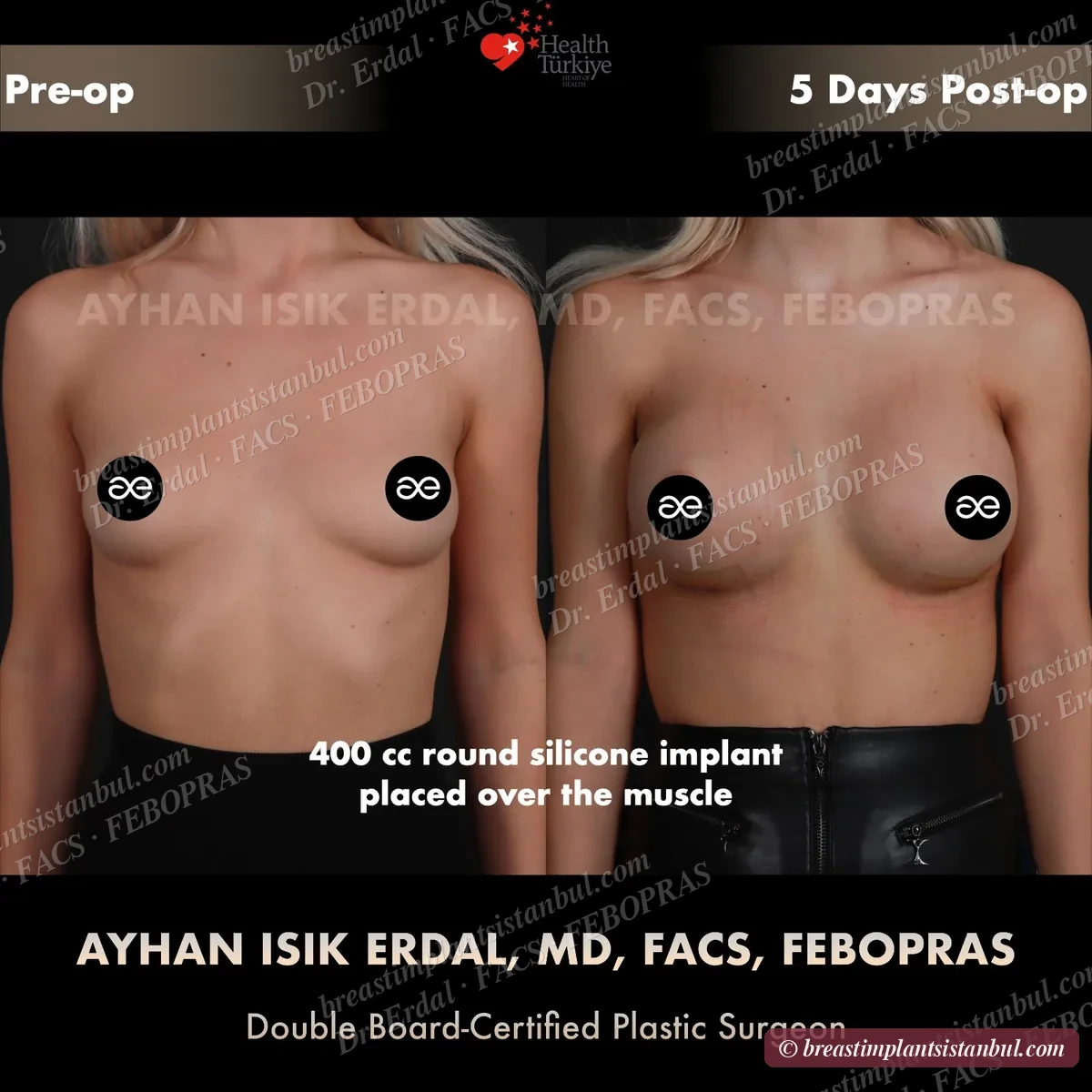
| Subglandular | Implant over the pectoralis muscle | Faster recovery, less initial discomfort | More visible implant edge in thin patients; higher historical contracture rates |
| Submuscular | Implant under the pectoralis muscle | Better soft tissue coverage, lower contracture rates, better mammography | Initial animation deformity (movement during pec contraction) |
| Dual plane | Upper portion submuscular, lower portion released | Combines submuscular coverage with natural lower pole drape | Technically more complex than either pure approach |
| Subfascial | Under the deep fascia, over the muscle | Some additional coverage vs subglandular without submuscular animation | Less commonly used; controversial whether truly distinct from subglandular |
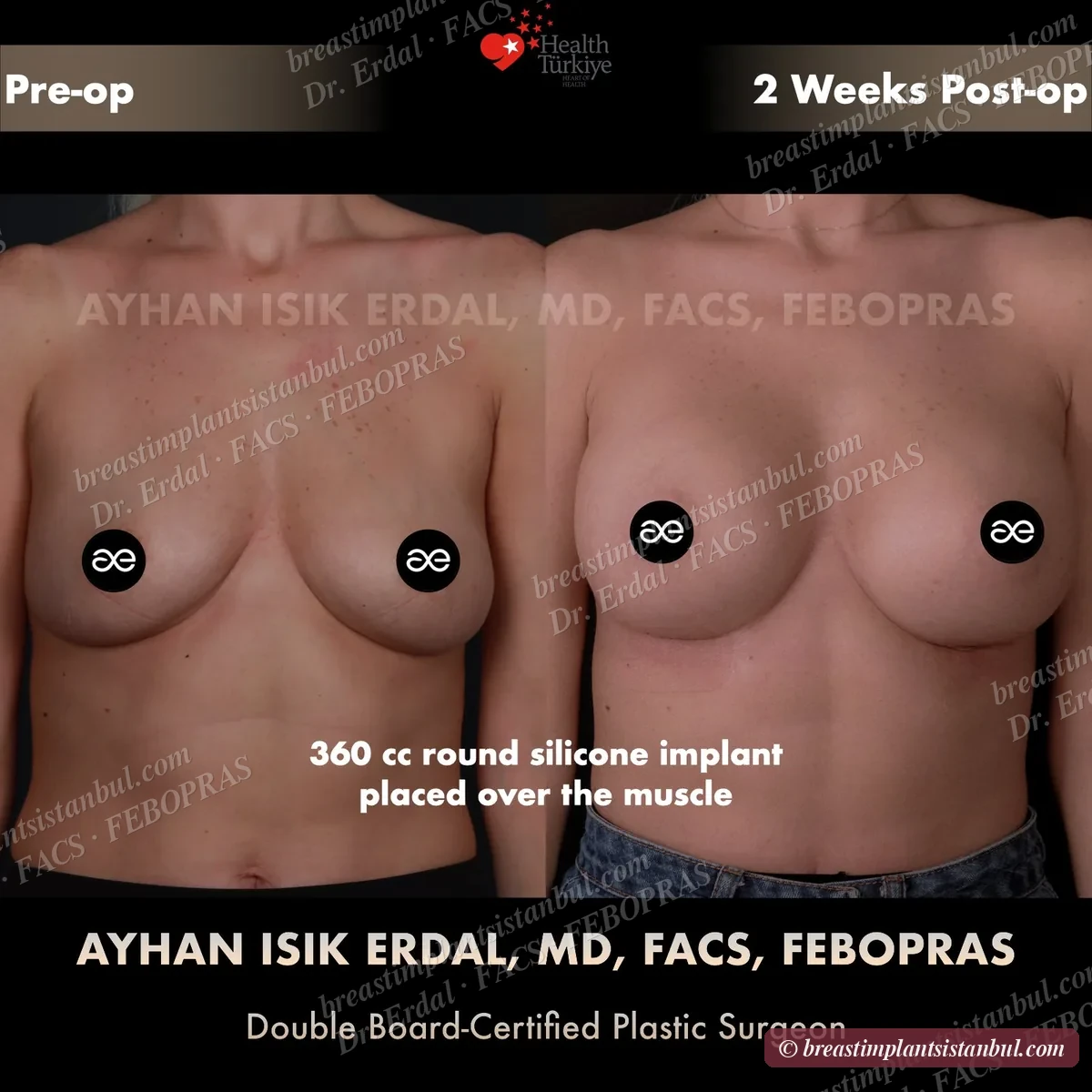
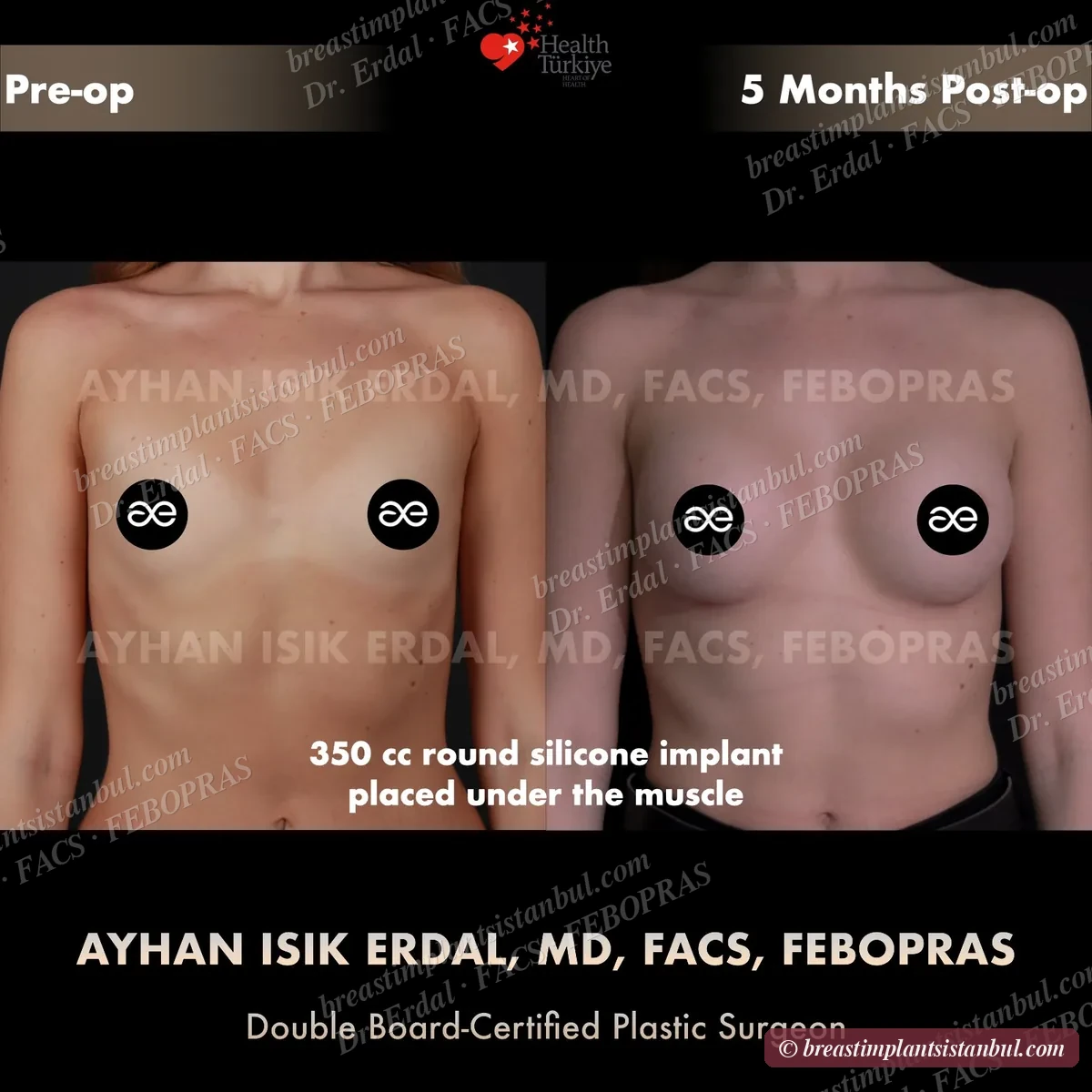
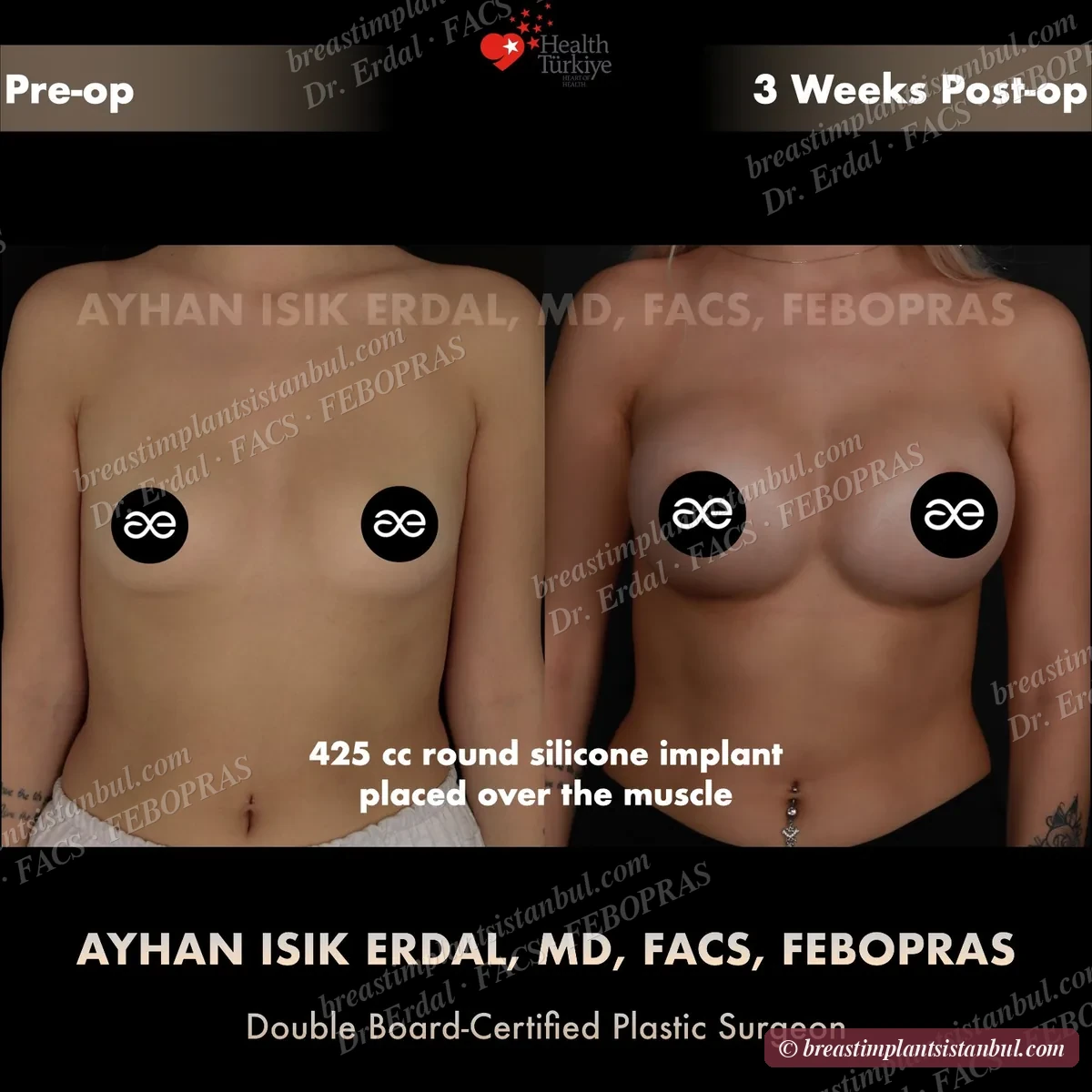
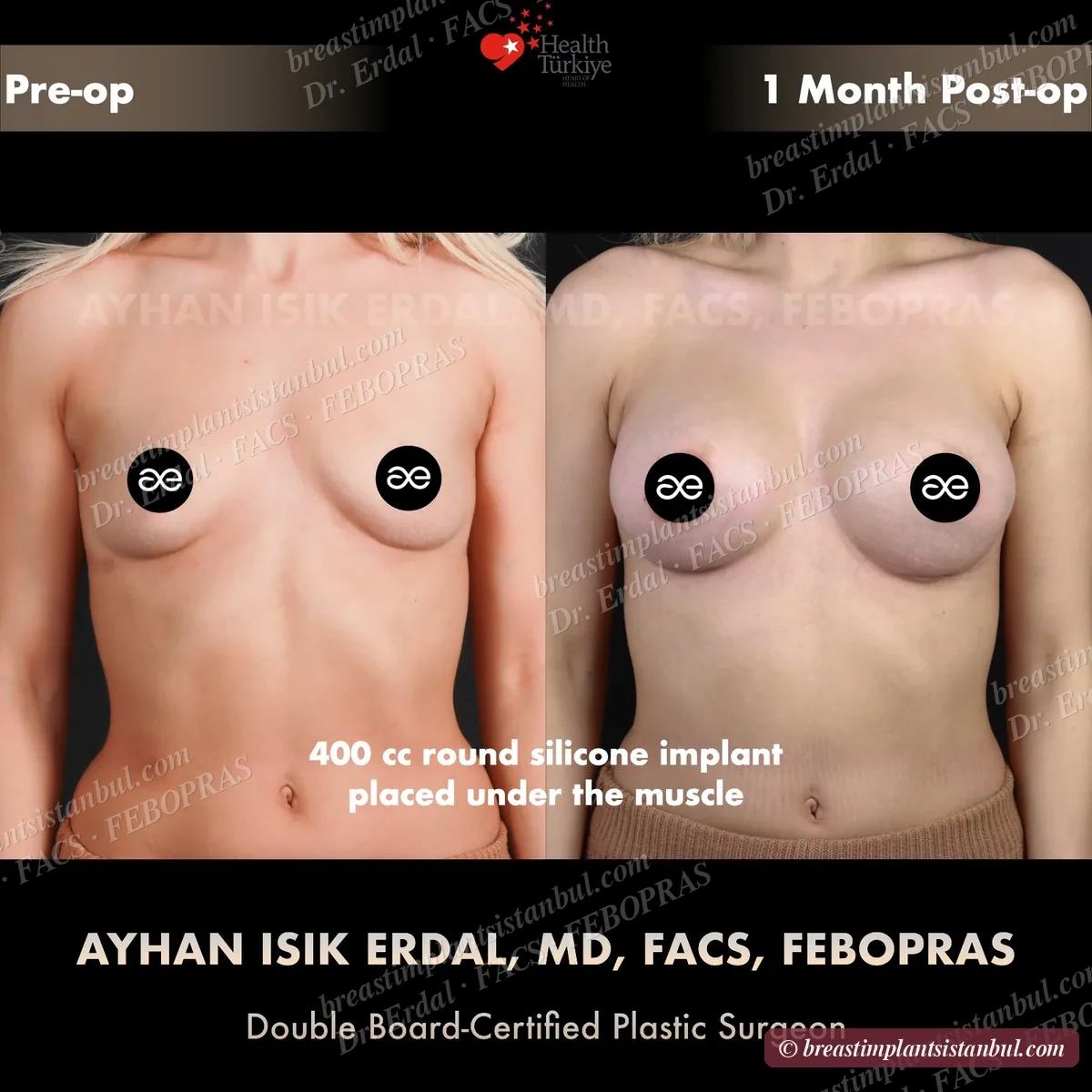
Dual-plane placement is the most common in modern practice for primary augmentation in patients with thin-to-moderate overlying tissue. Pure submuscular is preferred for very thin patients where maximum coverage is needed. Subglandular is reserved for specific cases (athletes concerned about animation deformity, patients with very generous overlying tissue).
Surgical technique
Incision options
- Inframammary fold (IMF): 4-5 cm incision in the natural fold under the breast. Most common — provides direct access for any implant size, well-hidden scar, allows precise pocket dissection.
- Periareolar: incision along the lower edge of the areola. Minimally visible scar but limits implant size and may affect nipple sensation; not preferred for large implants.
- Transaxillary: incision in the armpit. No breast scar but limited visualisation; not preferred for textured implants or large pockets.
- Transumbilical (TUBA): through the navel. Saline only; rarely used in modern practice.
IMF (inframammary fold) is the dominant technique in modern primary augmentation. Periareolar reserved for specific indications. Transaxillary and transumbilical are now uncommon.
Operative time
- Standard primary augmentation: 60-90 minutes operative time.
- General anaesthesia with experienced plastic surgery anaesthesia team.
- Day surgery in most cases — morning admission, evening or next-morning discharge.
Recovery timeline
All-inclusive cost
All-inclusive packages cover surgeon's fees, JCI-accredited hospital, anaesthesia, pre-op tests, hotel 5-7 nights, VIP airport transfers, surgical bra, all in-Istanbul follow-up visits, and 12-month remote follow-up. Specific implant brand/specifications affect the package level. Combined operations (e.g., aug + mastopexy) priced separately on the augmentation + mastopexy page.
For comparison: UK private breast augmentation typically £6,500-£9,500 (cosmetic only — NHS does not cover); German private €7,000-€10,000; US private $10,000-$15,000. The Turkey price reflects healthcare economics, not lower quality — JCI-accredited hospital, FACS/FEBOPRAS surgeon, modern implants from same global brands.
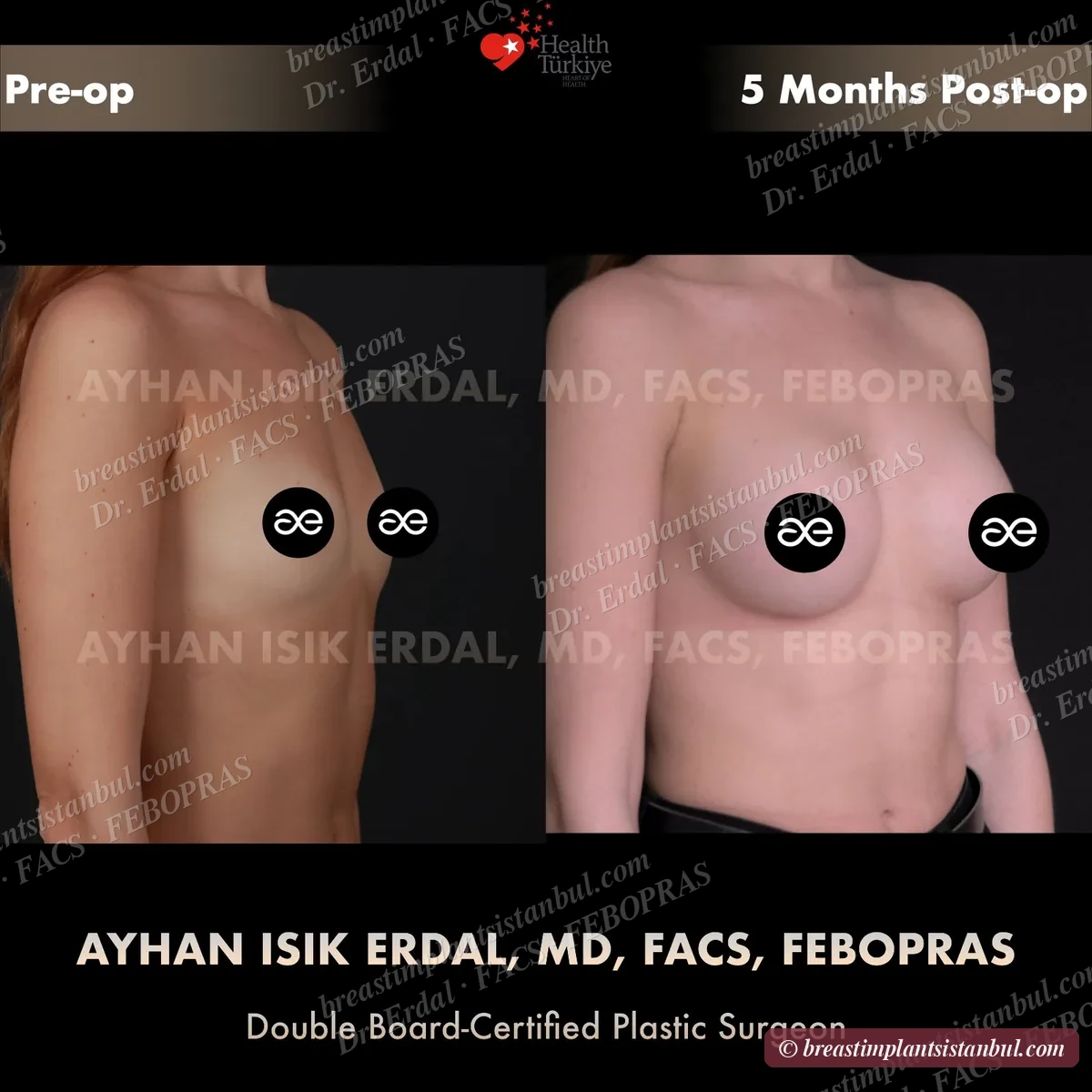
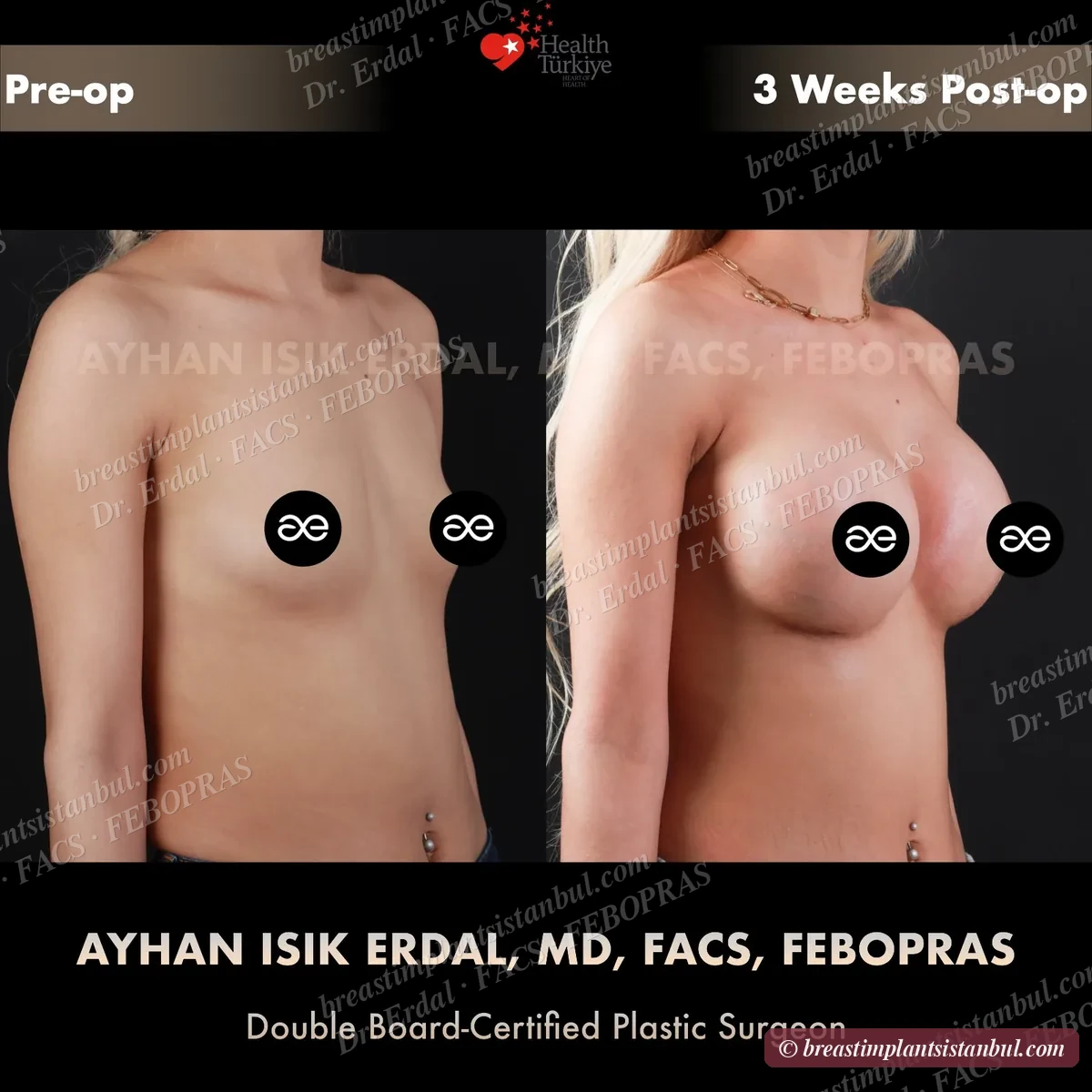
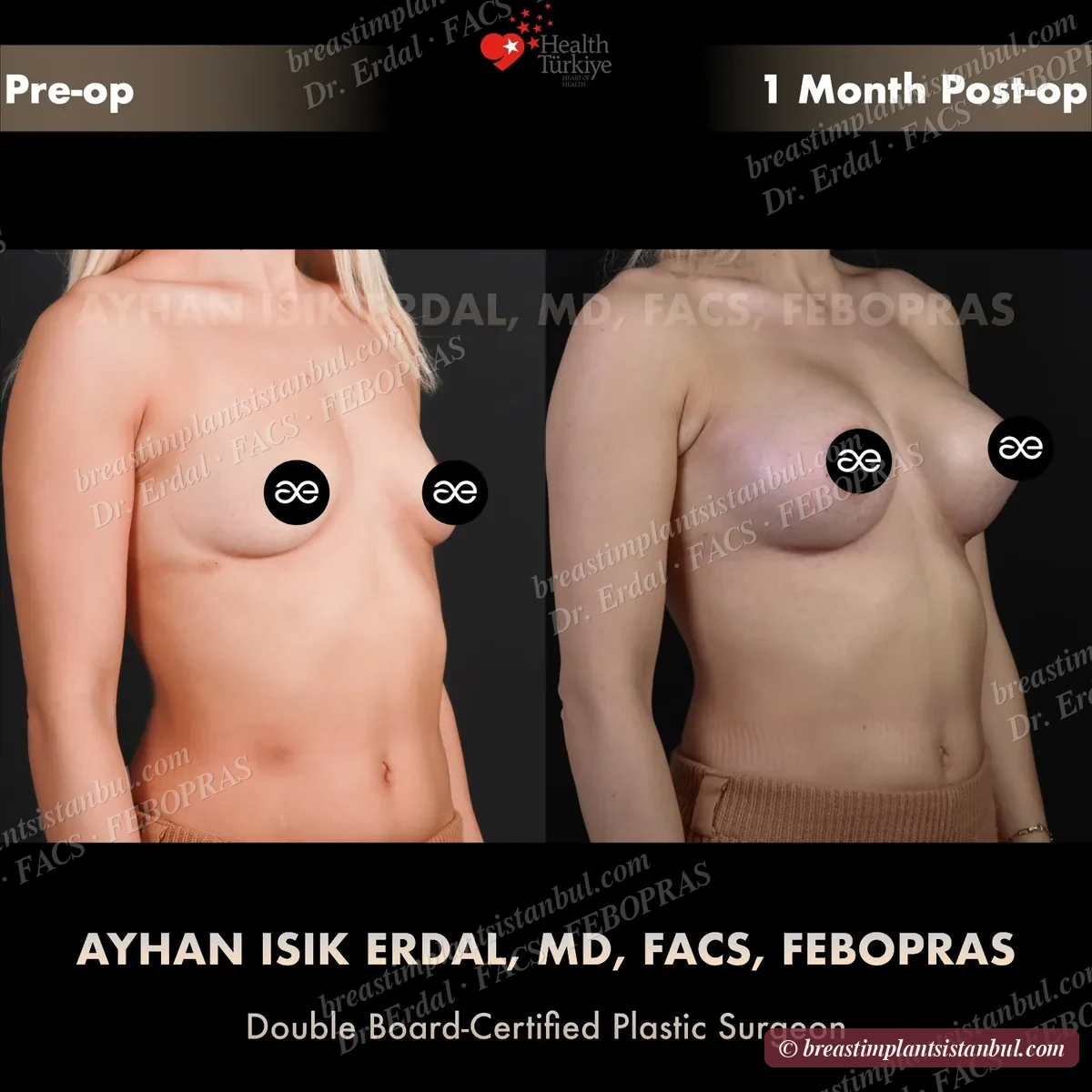
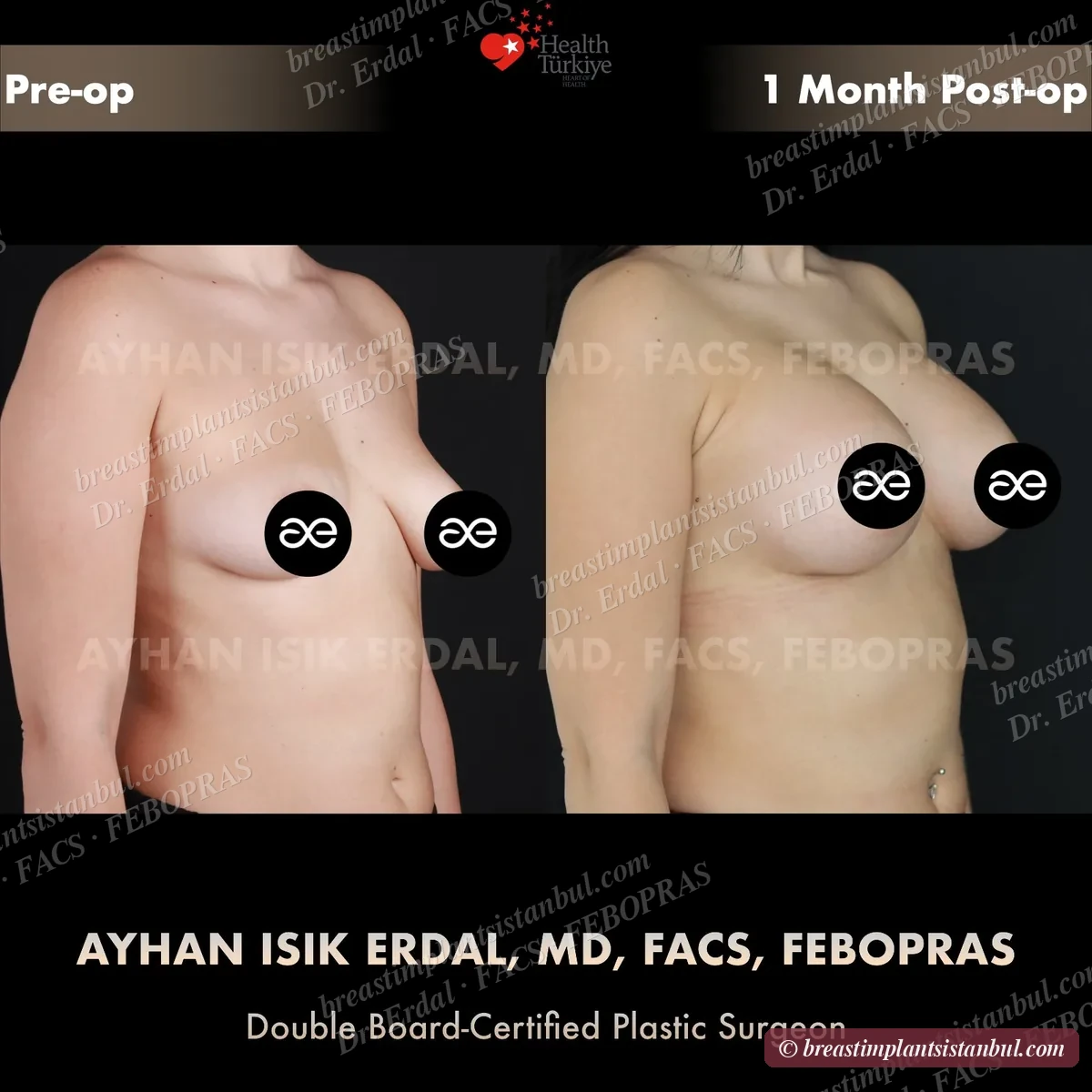
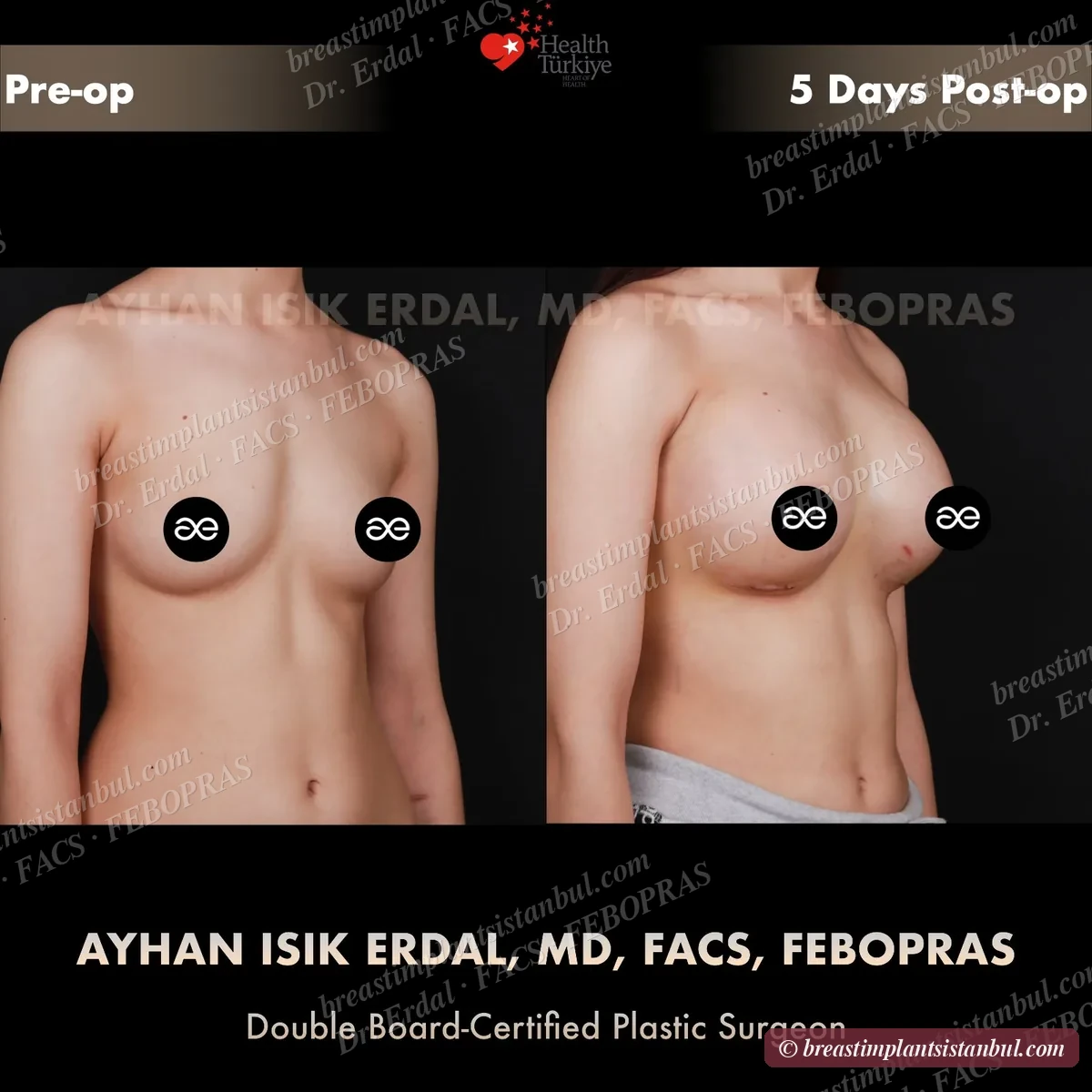
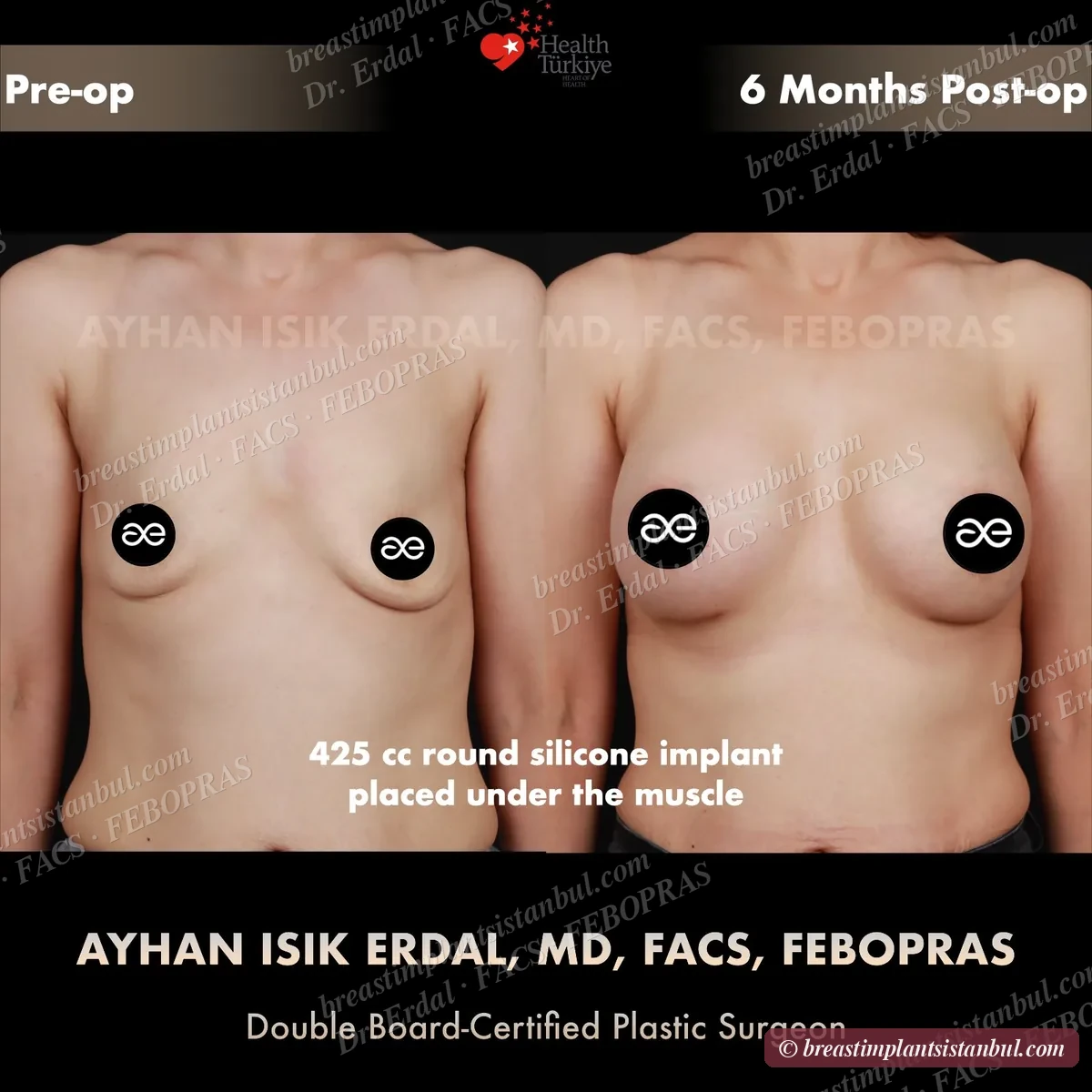
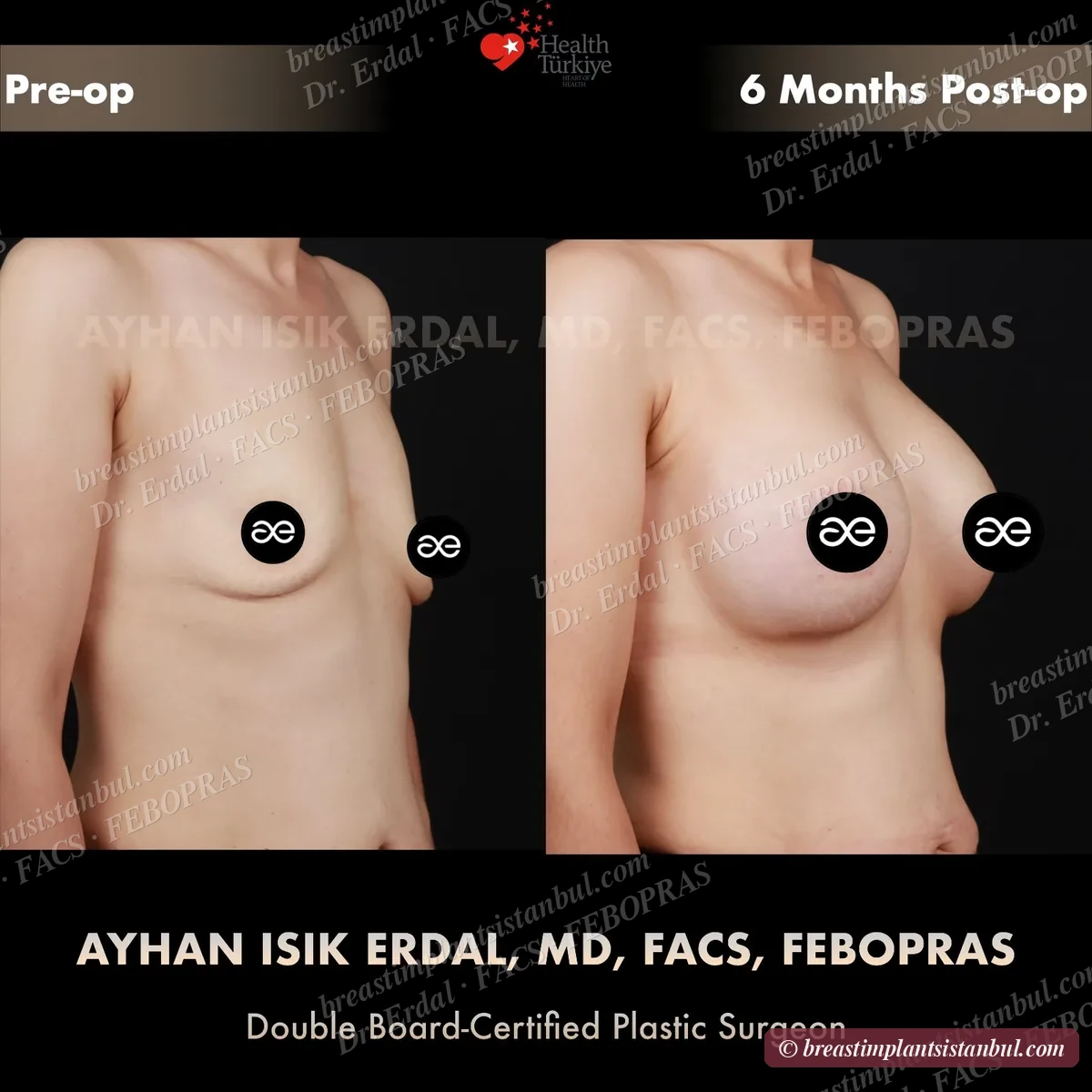
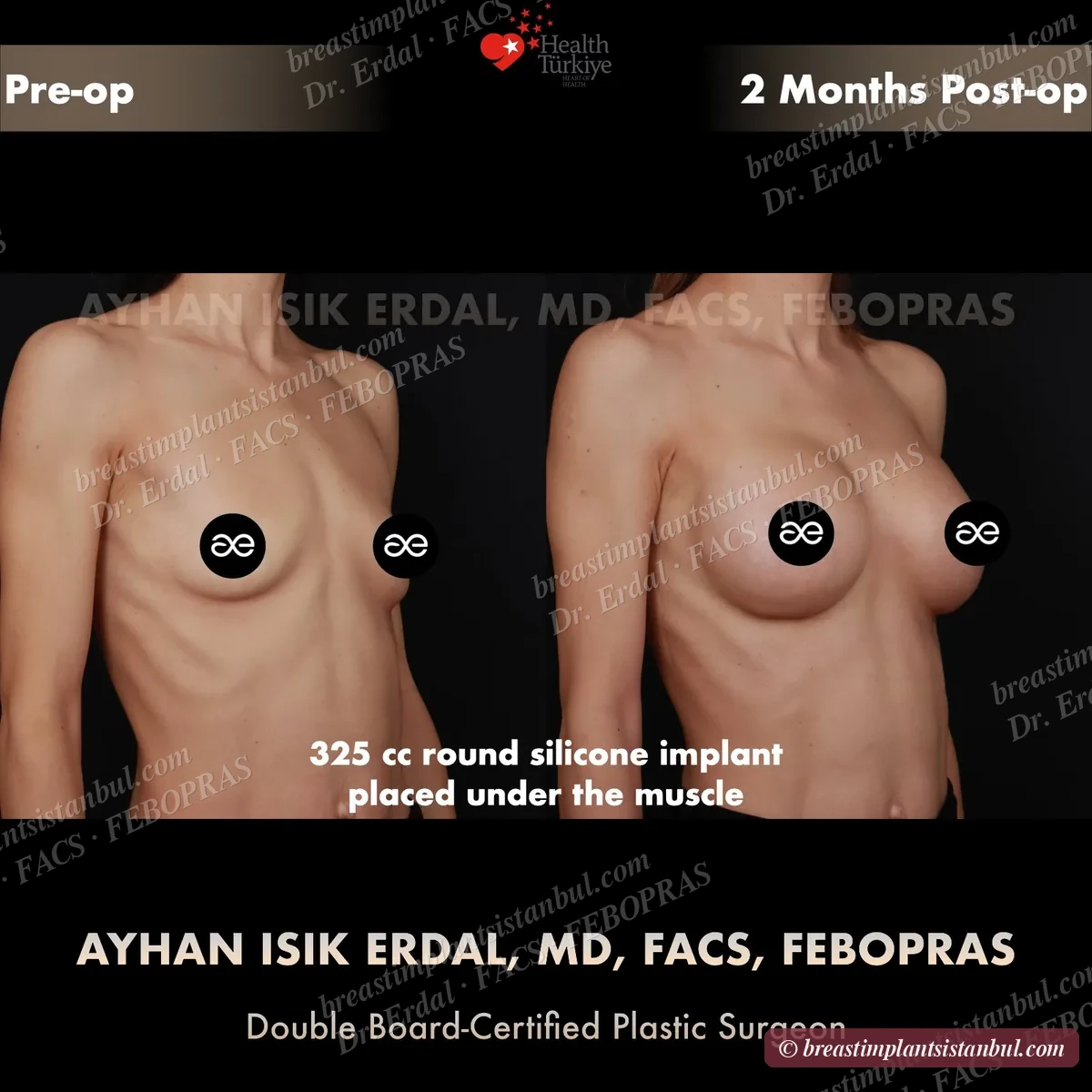
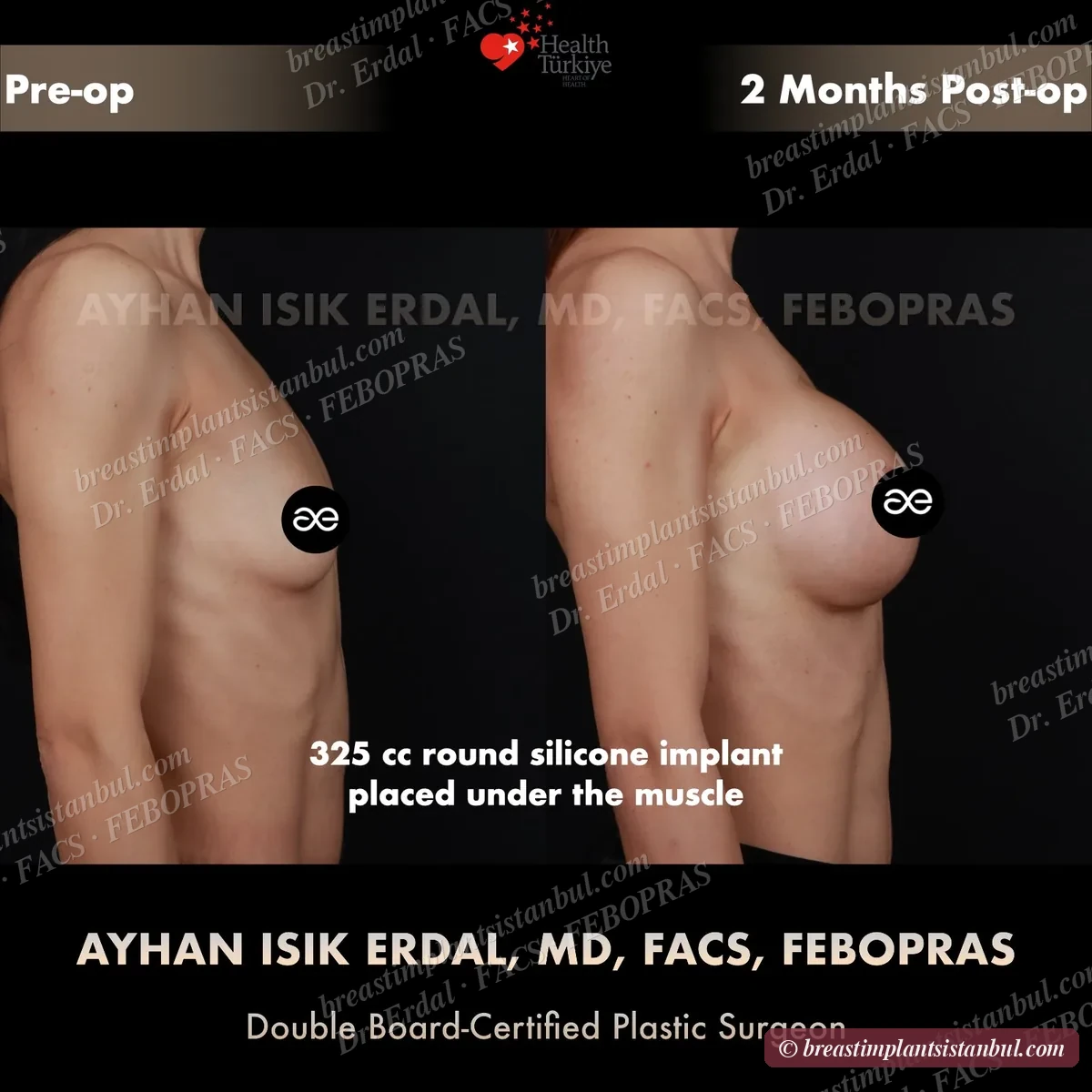
10-case before & after gallery
Each case shows three angles. All cases performed by Dr. Erdal at the JCI-accredited operating hospital. Implant specifications shown on each image. Recent results — full follow-up at 6+ months for final shape settling.